
Eastern Airlines Flight 401 departed John F. Kennedy International Airport on the evening of December 29, 1972, bound for Miami International Airport. The aircraft was a Lockheed L-1011 TriStar, one of the most technologically advanced widebody jets in commercial service, delivered to Eastern Airlines less than a year earlier. Captain Robert Loft, a veteran with nearly 30,000 flight hours, was in command, with First Officer Albert Stockstill and Second Officer Donald Repo comprising a crew of considerable combined experience. The flight was uneventful. The approach to Miami was normal. Then, as Stockstill lowered the landing gear on descent, a small green indicator lamp in the nose gear position circuit failed to illuminate.
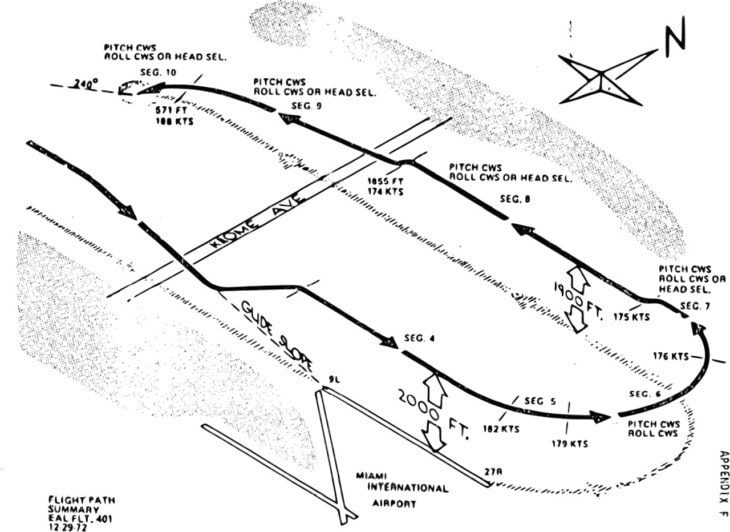
The light was supposed to confirm that the nose landing gear was down and locked. Without it, Captain Loft could not verify the nose gear position. He broke off the approach, put the aircraft into a shallow holding pattern at 2,000 feet over the dark Florida Everglades west of Miami, and the crew began to investigate. Over the next several minutes, the cockpit became consumed by the indicator problem.
Captain Loft, First Officer Stockstill, Second Officer Repo, and Angelo Donadeo, a maintenance technician riding in the jumpseat on a deadhead trip, all focused on the same small lamp. At some point during this period, the autopilot’s altitude hold function disengaged, most likely when someone leaned against the control column without registering what had happened. Nobody noticed. The aircraft began a slow, barely perceptible descent from 2,000 feet. Nobody was watching the altimeter. An altitude alert briefly sounded, but in the crowded cockpit with every mind trained on the gear indicator, nobody processed it in time to act.
Flight 401 struck the surface of the Florida Everglades at 11:42 p.m. at approximately 227 miles per hour. The aircraft disintegrated on impact across the flat, wet terrain. Of the 176 people on board, 101 were killed. Seventy-five survived, many seriously injured, and were pulled from the swamp by airboats and helicopters during a nighttime rescue operation that continued until the early hours of December 30. The accident was, at the time, among the deadliest in US aviation history. It was also one of the most preventable: the aircraft had been fully functional, the crew experienced, the weather clear, and the Everglades were flat and gave no terrain warning whatsoever.

What the NTSB found: a cockpit absorbed in a problem that did not exist
The NTSB investigation established a finding that is striking even now: the nose gear, the object of every person’s attention in those final minutes, had never been the problem. The landing gear was down and locked throughout the approach and the hold. What had failed was the indicator circuit itself: a burned-out bulb or an electrical fault in the position indicating system.
The aircraft was fully capable of landing safely from the moment the light failed to illuminate. Every one of the 101 people who died in the Everglades that night died not because of any meaningful mechanical failure, but because the crew’s entire cognitive attention was occupied by a false alarm, and no one was watching what the aircraft was doing.
The NTSB probable cause finding was direct: “The Board determines that the probable cause of this accident was the failure of the flightcrew to monitor the flight instruments during the final 4 minutes of flight, and to detect an unexpected descent soon enough to prevent impact with the ground. Preoccupation with a malfunction of the nose landing gear position indicating system distracted the crew’s attention from the instruments and allowed the descent to go unnoticed.”
The investigation identified the autopilot disconnect as a critical element: the altitude hold had been deactivated, probably by inadvertent contact with the control column, and the crew had no indication in the darkness over featureless terrain that the aircraft had begun to descend. The L-1011’s altitude alerting system had functioned correctly. It produced a warning as the aircraft departed its assigned altitude. The warning was not acted upon.












The moment the descent became fatal
The cockpit voice recorder captured a crew member recognizing the altitude loss at approximately 90 seconds before impact. Attempts to arrest the descent began, but the aircraft was already too low over flat, dark terrain with no visual references to enable recovery. Flight 401 had descended from 2,000 feet at roughly 200 feet per minute over four minutes: a rate so gradual it produced no unusual sensation, and only visible on instruments nobody had been watching. The nose gear indicator, throughout, was showing the same faulty reading it had been showing all along.
21:20
Departure from JFK. Eastern Airlines Flight 401 lifts off from New York bound for Miami with 176 people on board. Captain Robert Loft commands a Lockheed L-1011 TriStar, one of the newest widebody jets in commercial service.
23:02
Descent toward Miami begins. The crew initiates a routine descent toward Miami International Airport. The approach is normal. Weather is clear.
23:34
Gear extended, indicator fails. First Officer Stockstill lowers the landing gear. The nose gear position indicator light does not illuminate. Captain Loft breaks off the approach and establishes a holding pattern at 2,000 feet over the Everglades to investigate.
23:38
Altitude alert sounds, unheeded. The aircraft’s altitude alerting system briefly warns that the aircraft has descended from its assigned altitude. Every person in the cockpit is focused on the gear indicator. The alert is not acted upon.
23:40
Descent recognized. A crew member calls out that the aircraft has lost altitude. The aircraft is well below 2,000 feet and still descending at approximately 200 feet per minute over flat, dark terrain.
23:42
Impact. Flight 401 strikes the Florida Everglades at approximately 227 miles per hour. Of 176 on board, 101 are killed and 75 survive. The nose gear, throughout, had been down and locked.
How Eastern 401 put a ground proximity warning on every commercial aircraft
By the early 1970s, the FAA was already examining what investigators called controlled flight into terrain: the pattern in which fully functional aircraft, with functioning engines and experienced crews, flew into the ground because the crew was not monitoring altitude or terrain proximity. A cluster of CFIT accidents in the late 1960s and early 1970s had established a grim pattern.
Eastern 401 was the most prominent: a major US carrier, a new and technically sophisticated aircraft, a crew with no shortage of skill or experience. The NTSB’s safety recommendations from the investigation specifically called for a system that would warn crews when the aircraft was descending into dangerous proximity to terrain, independent of whether anyone in the cockpit was watching the instruments.
The FAA issued a Notice of Proposed Rulemaking in 1973, citing the Eastern 401 accident and related CFIT events. The final rule requiring Ground Proximity Warning Systems on large turbine transport aircraft operated under 14 CFR Part 121 was published and became effective December 1, 1975, codified as 14 CFR 121.360. GPWS units, developed primarily by Don Bateman of Sundstrand Data Control (later Honeywell), work by continuously monitoring flight parameters associated with dangerous proximity to terrain.
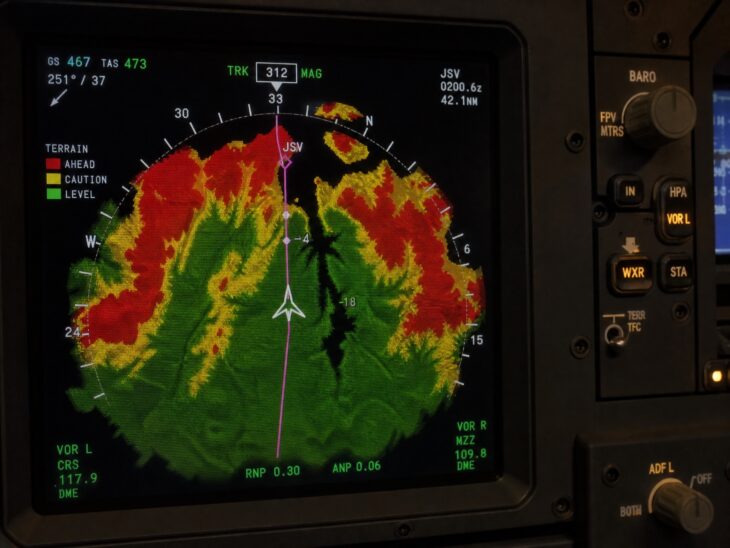
The system detects: excessive sink rate; excessive terrain closure rate; loss of altitude shortly after takeoff or go-around; unsafe terrain clearance when the landing gear or flaps are not in a landing configuration; and unsafe descent below an instrument landing system glideslope. When any of these conditions are detected, a voice alert fires automatically: “Sink rate.” “Pull up.” “Terrain, terrain.” The crew does not have to notice the altimeter. The aircraft tells them, loudly and repeatedly, that something is wrong with where they are relative to the ground.
The GPWS requirement was progressively extended. The FAA amended 14 CFR 121.360 to encompass a wider range of aircraft. ICAO Annex 6, Part I, was amended to require ground proximity warning equipment on turbine-powered aircraft exceeding specified weight thresholds, with the requirement phased in for both new and existing aircraft during the late 1970s and 1980s.
National aviation authorities across Europe, Canada, Australia, and beyond adopted equivalent requirements. In the 1990s, Enhanced GPWS (EGPWS), also developed by Don Bateman and Honeywell, added a digital terrain database and look-ahead capability. Where the original GPWS could only warn of a dangerous condition already present, EGPWS projects the aircraft’s current trajectory forward against a global terrain map and can detect potential terrain conflict from miles away, providing warnings that give the crew minutes rather than seconds to react.
The FAA mandated Terrain Awareness and Warning Systems (TAWS, the category that includes EGPWS and equivalent systems) on turbine aircraft with six or more passenger seats operated under Part 121, under 14 CFR 121.354, with the rule phased in through the early 2000s. An equivalent rule applied to Part 135 operators under 14 CFR 135.154.
The effect on controlled flight into terrain accident rates has been significant and documented. Before GPWS was widespread, CFIT was among the leading causes of fatal airline accidents worldwide. A 1999 FAA safety analysis estimated that GPWS had already prevented hundreds of accidents and saved thousands of lives since its introduction.
In the decades that followed, CFIT fatalities on GPWS-equipped and EGPWS-equipped aircraft fell dramatically as a proportion of total aviation accidents. The pattern of an experienced crew on a functioning aircraft descending into flat terrain while preoccupied with a cockpit problem has become exceptionally rare on aircraft with modern terrain warning systems.
The FAA simultaneously strengthened altitude alerting requirements under 14 CFR 121.356, requiring turbine aircraft to carry systems that alert crews when deviating from a selected altitude, and updated crew training standards to make altitude alert response a mandatory trained procedure. The L-1011 had an altitude alerting system on the night of December 29, 1972. It worked. What was missing was the system that would not let the crew ignore it.
What changed because of Eastern Airlines Flight 401
Ground Proximity Warning System mandated on all large turbine transport aircraft under Part 121 (14 CFR 121.360), effective December 1, 1975. ICAO Annex 6 amended to require terrain warning equipment internationally. Enhanced GPWS (EGPWS) and Terrain Awareness and Warning Systems (TAWS) subsequently mandated under 14 CFR 121.354, adding look-ahead terrain database capability. Altitude alerting system requirements strengthened under 14 CFR 121.356. CFIT accident rates on GPWS-equipped and EGPWS-equipped aircraft fell substantially in the decades following the mandates.
Eastern Airlines Flight 401 is often summarized as a distraction accident, but the investigation’s lasting contribution was more precise than that label suggests. The accident did not happen because the crew was negligent or under-qualified. It happened because aviation had not yet built the systems necessary to protect a crew whose full attention was genuinely consumed by a real problem, however minor that problem turned out to be.
In 1972, no rule required a captain to keep scanning the altimeter while troubleshooting a gear indicator. No independent system would alert him if he did not. That gap was the underlying failure. What the accident produced was a requirement: every commercial airliner now carries a system that monitors terrain proximity continuously, independent of what the crew is focused on, and that makes itself heard regardless of whether the crew is ready for the warning.
The human pattern at the center of this accident, a cockpit absorbed in one problem while another develops unobserved, runs through aviation history in different contexts and with different outcomes. The most direct parallel is United Airlines Flight 173, which crashed in Portland just six years later under nearly identical circumstances: the same gear indicator fixation, the same failure of the crew to maintain situational awareness about a developing emergency.
That accident produced a different change, one focused on how crews communicate rather than how aircraft warn, and it is the origin story of Crew Resource Management training. For the full record of the accidents that remade commercial aviation safety, the complete series is at The Flights That Changed Aviation.
FAQ
Sources and references used for research and fact-checking.
- Aircraft Accident Report: Eastern Air Lines, Inc., L-1011, N310EA, Miami, Florida, December 29, 1972 - National Transportation Safety Board
- 14 CFR 121.360 — Ground proximity warning systems - Federal Aviation Administration / Code of Federal Regulations
- 14 CFR 121.354 — Terrain awareness and warning systems - Federal Aviation Administration / Code of Federal Regulations
- Ground Proximity Warning System (GPWS) - SKYbrary
- Controlled Flight Into Terrain (CFIT) - SKYbrary
About the Author

Tim is the owner and editor-in-chief of AeroCorner, where he has spent the last seven years overseeing aviation content covering aircraft, airlines, airports, and the broader aviation industry. Through years of researching, editing, and publishing aviation-focused content, he has developed extensive practical knowledge of commercial aviation and air travel. Based in Asia and a frequent traveler himself, Tim also brings firsthand passenger experience to AeroCorner’s coverage. Outside of publishing, he has also explored aviation firsthand through hands-on flight training in New Zealand.